Join Clinicians Worldwide
Evidence-based insights to enhance hearing care—twice a month
Subscribe Now Evidence-based insights to enhance hearing care—twice a month
Subscribe Now
Max Schnabl
Published Jun 15, 2026
Renowned ENT surgeon Prof. Paul Van de Heyning argues that low frequencies, long electrodes, and anatomy-based fitting can reshape cochlear implant care. Find the key messages of his lecture at Johns Hopkins University School of Medicine in this article—and watch the embedded recording of his presentation for full information.

In this lecture, Prof. Van de Heyning presents a strong case that the importance of low-frequency hearing, generally below 450 Hz, has been underestimated in both hearing science and cochlear implant practice.
On standard audiograms, these frequencies appear only in a small area and are often not included in widely used pure-tone averages. As a result, they are not only underexposed, in his words, but also underappreciated.
The talk’s central message is that low frequencies are essential for natural hearing and should be much better preserved or restored in cochlear implant users. According to Prof. Van de Heyning, this requires a change in how clinicians think about the cochlea, how electrodes are selected and inserted, and how implants are fitted after surgery.
His argument rests on three core ideas:
Prof. Van de Heyning stresses how much low frequencies contribute to normal hearing. They are important for the naturalness of sound, timbre, prosody, intonation, and emotional expression in speech. They help listeners distinguish between male and female voices, separate one conversation from another, and understand speech in noisy environments.[1][2][3][4][5]
They are also central to music perception, particularly the appreciation of sound quality and fullness, and to awareness of the surrounding spatial soundscape. These are not small refinements. The low frequencies shape how people experience voices, environments, and music in everyday life.
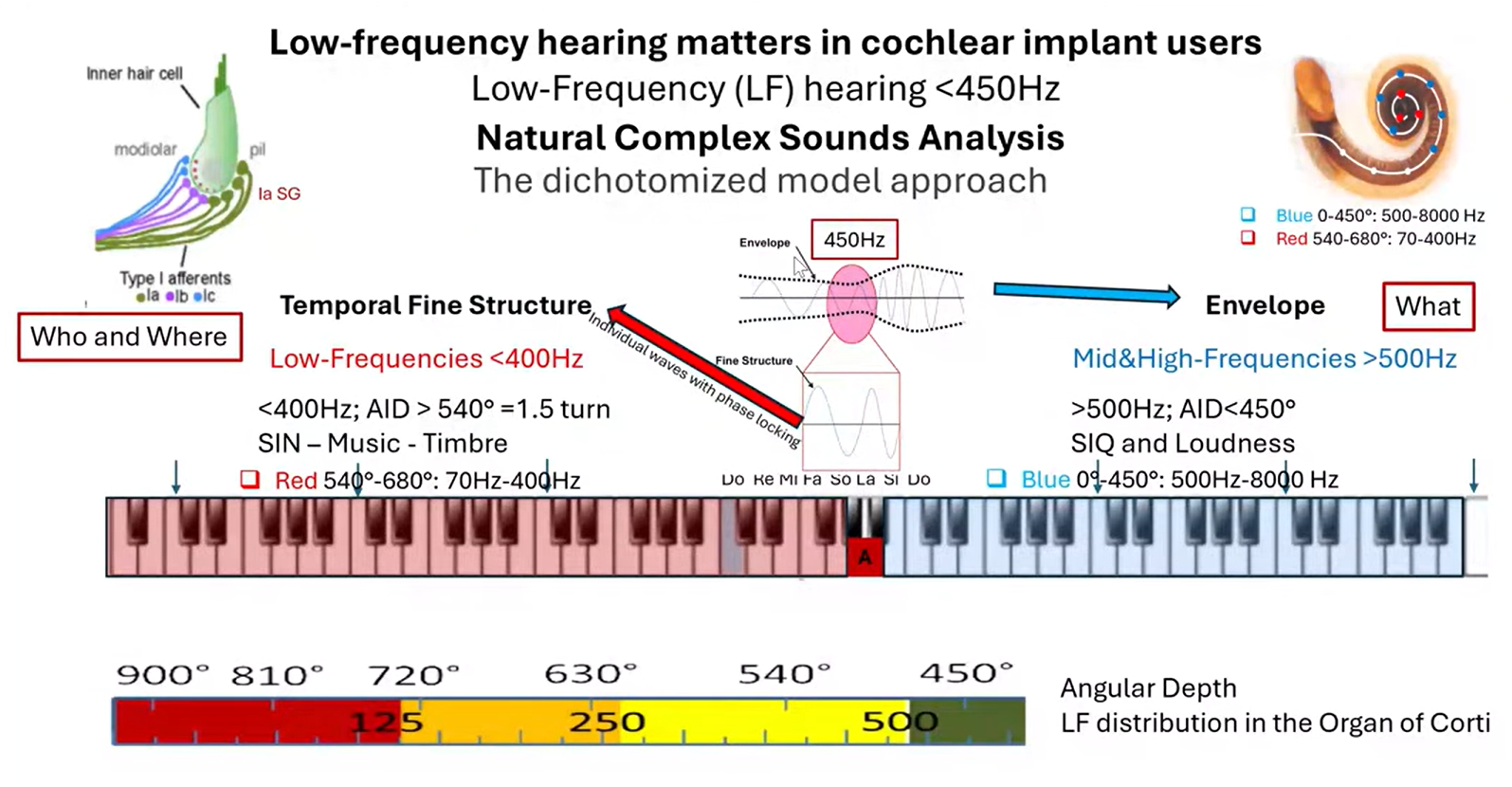
To illustrate the extent and importance of low frequencies, Van de Heyning uses the image of a piano keyboard. The reference tone (“standard pitch”) A at 440 Hz sits around the middle, and everything below it makes up about half of the keyboard.
Mapping this onto the cochlea with the Greenwood function shows that a substantial portion of the cochlea is devoted to these lower tones. This stands in contrast to their minor appearance on the audiogram.
The lecture then turns to the physiology of hearing. The cochlea breaks complex sounds into multiple narrow-band signals. Each of these signals contains two main features:
Van de Heyning explains that in the mid and high frequencies, especially above about 500 Hz, speech understanding in quiet is dominated by the envelope. This helps listeners recognize what is being said and contributes to loudness perception.
In contrast, in the low frequencies, the dominant cue is the temporal fine structure, which is transmitted in the auditory system through phase locking. This fine structure is especially important for identifying who is speaking, where sound is coming from, hearing speech in noise, and appreciating music and timbre.
This distinction matters because conventional cochlear implant strategies largely rely on envelope information and place coding. But if low-frequency hearing depends heavily on temporal fine structure, then those low tones require a different kind of stimulation.
A central argument of the lecture is that low-frequency hearing cannot be restored unless the implant electrode array actually reaches the respective part of the cochlea. Prof. Van de Heyning focuses on the apical region beyond one and a half turns, or about 540° angular insertion depth.
He cites data showing that 24 mm electrodes or shorter generally do not reach this low-frequency region. 28 mm electrodes reach it in some but not all patients, whereas 31 mm electrodes do so much more consistently.[5][6][7]
“Almost half of the cochlea is dedicated to perceiving low tones. (…) If we use electrodes of 22 mm or shorter, it is as if we ask a pianist to play the piece only on the right half of the piano.”
Prof. Paul Van de Heyning
This is why he rejects a “one-size-fits-all” approach. Cochleae vary in size, so electrode length should be selected individually. He describes the use of imaging and planning software such as OTOPLAN, which allows clinicians to measure cochlear size and visualize electrode positions before surgery.
According to Van de Heyning, cochlear implant users with short electrodes are essentially asked to hear with only the “right half” of the piano. Low-frequency information is squeezed into a smaller space, resulting in compression and distortion.
In the apex, pitch is more strongly linked to rate coding, similar to the way phase locking conveys low-frequency information in normal hearing. In the base of the cochlea, traditional place coding remains dominant.
This finding leads Van de Heyning to conclude that if clinicians want to restore clear low-frequency pitch below about 400-450 Hz, they must stimulate the apical region of the cochlea and do so with a coding strategy based on stimulation rate, not only on electrode position.
“To be able to stimulate low tones, we need the apical electrode located beyond one and a half turns.”
Prof. Paul Van de Heyning
A major practical problem in cochlear implantation is frequency-place mismatch. This happens when the processor sends a sound frequency to an electrode located in a cochlear region that corresponds to a different frequency.[5]
Prof. Van de Heyning gives the example of a low incoming tone around 120 Hz being assigned to an electrode physically situated around the 590 Hz place. The patient then perceives a low tone as unnaturally high.
This helps explain why some cochlear implant users report “Mickey Mouse” voices. Such mismatch affects more than sound quality: The larger the mismatch, the poorer the speech scores and the slower the adaptation after fitting. It also distorts the distinction between male and female voices and undermines the emotional content of speech.[7][8][9][10]
Longer electrodes reduce mismatch because they reach lower-frequency cochlear regions. But they do not eliminate it on their own. This is why Van de Heyning is a proponent of anatomy-based fitting (ABF): It uses postoperative imaging to determine the actual location of each electrode and then adjusts the frequency allocation map to match the patient’s individual cochlear anatomy. Several studies show that CI users prefer anatomy-based fitting over default fitting, especially when listening to music.[11][12]
Prof. Van de Heyning argues that low frequencies (below 450 Hz) represent a major part of hearing: They are essential for voice identity, emotion, music, and listening in noise.
To provide CI hearing that is as close as possible to natural hearing, he suggests the following steps:
His closing metaphor is simple and memorable: Hearing is not restored if patients are given only half the piano. But even with the full keyboard, success still depends on hitting the right notes. For Prof. Van de Heyning, the future of cochlear implants lies in doing both: restoring access to the low frequencies and matching them correctly to the cochlea so that hearing becomes not just functional, but closest to natural.
Dr. Paul Van de Heyning is emeritus professor and former dean of the Faculty of Medicine and Health Sciences at the University of Antwerp. As an active consultant and former head of the Department of Otorhinolaryngology and Head and Neck Surgery at Antwerp University Hospital, he is one of the world’s leading experts on inner ear pathologies and cochlear implantation. Prof. Van de Heyning is founding member, past chair, and current vice-chair of the HEARRING group.
Subscribe to the MED-EL Professionals Blog and receive articles about MED-EL products, case studies, hearing implant surgeries, and rehabilitation materials sent directly to your inbox.
References
Roy et al. 2016. Deeper cochlear implant electrode insertion angle improves detection of musical sound quality deterioration related to bass frequency removal. Otology & Neurotology 37(2), 146-151.
Park et al. 2025. Benefits of Cochlear Implantation and Hearing Preservation for Children With Preoperative Functional Hearing: A Prospective Clinical Trial. Ear & Hearing 46(4), 941-951.
Todd et al. 2017. Encoding a Melody Using Only Temporal Information for Cochlear-Implant and Normal-Hearing Listeners. Trends in Hearing 2017(21), 1-15.
Carlyon et al. 2025. Limitations on Temporal Processing by Cochlear Implant Users: A Compilation of Viewpoints. Trends in Hearing 29 2025,1-39.
Li et al. 2025. The cochlear apex demystified: Implications from synchrotron radiation phase-contrast imaging and microscopy for cochlear implantation. Journal of Anatomy 247(6), 1283-1296.
Li et al. 2021. Three-dimensional tonotopic mapping of the human cochlea based on synchrotron radiation phase-contrast imaging. Scientific Reports 11(1), 4437.
Canfarotta et al. 2020. Frequency-to-place mismatch: Characterizing variability and the influence on speech perception outcomes in cochlear implant recipients. Ear & Hearing 41(5), 1349-1361.
Canfarotta et al. 2020. Influence of Age at Cochlear Implantation and Frequency-to-Place Mismatch on Early Speech Recognition in Adults. Otolaryngology–Head and Neck Surgery 162(6), 926-932.
Dorman et al. 2019. Looking for Mickey Mouse™ but finding a munchkin: The perceptual effects of frequency upshifts for single-sided deaf, cochlear implant patients. Journal of Speech, Language, and Hearing Research 62, 3493-3499.
Dorman et al. 2024. Close approximations to the sound of a cochlear implant. Frontiers in Human Neuroscience 18.
Yang et al. 2022. Image-Guided Cochlear Implant Programming: A Systematic Review and Meta-analysis. Otology & Neurotology 43(9), 924-935.
Creff et al. 2024. Tonotopic and Default Frequency Fitting for Music Perception in Cochlear Implant Recipients: A Randomized Clinical Trial. JAMA Otolaryngology–Head & Neck Surgery 150(11), 960-968.
References
Max Schnabl
Max Schnabl, Mag. BA, is part of the MED-EL Professionals Blog editorial team. A trained journalist, Max has specialized in writing about hearing solutions since 2017. He enjoys communicating new innovations and surgical techniques to hearing professionals.
Was this article helpful?
Thanks for your feedback.
Sign up for newsletter below for more.
Thanks for your feedback.
Please leave your message below.
CTA Form Success Message
Send us a message
Field is required
John Doe
Field is required
name@mail.com
Field is required
What do you think?
The content on this website is for general informational purposes only and should not be taken as medical advice. Please contact your doctor or hearing specialist to learn what type of hearing solution is suitable for your specific needs. Not all products, features, or indications shown are approved in all countries.
Max Schnabl
Max Schnabl, Mag. BA, is part of the MED-EL Professionals Blog editorial team. A trained journalist, Max has specialized in writing about hearing solutions since 2017. He enjoys communicating new innovations and surgical techniques to hearing professionals.
Get the latest research and resources to help people with every kind of hearing loss. Subscribe to the MED-EL Professionals Blog now.
Registration was successful
We’re the world’s leading hearing implant company, on a mission to help people with hearing loss experience the joy of sound.
Find your local MED-EL team
The content on this website is for general informational purposes only and should not be taken as medical advice. Please contact your doctor or hearing specialist to learn what type of hearing solution is suitable for your specific needs. Not all products, features, or indications shown are approved in all countries.