
MED-EL
Published May 24, 2018
Tip Fold-Over: Perimodiolar Cochlear Implant Electrode Arrays

Even in a profoundly deafened cochlea, there is intricate network of living and active neural structures. If a cochlear implant electrode array deviates from the scala tympani to the scala vestibuli, a toxic inflammation can damage underlying auditory nerve structures.
As Professor Helge Rask-Andersen explained, this is why structure preservation surgery should be considered essential for every cochlear implant candidate, even if there is no residual hearing—a deaf cochlea is not a dead cochlea.
In fact, damage to the structures of the cochlea can result in significantly lower speech understanding and loss of residual hearing—clearly not an ideal outcome for any cochlear implant recipient.
One of the most significant factors in preserving cochlear structures is the design of the electrode array. Pre-curved perimodiolar arrays and mid-scala arrays can be far more likely to deviate through the basilar membrane into the scala vestibuli, which can cause extensive damage to the cochlea.1,2,3,4
However, there’s another issue to watch out for with pre-curved perimodiolar arrays. Today, we’re going to look at the mechanisms of tip fold-over in perimodiolar arrays, and how this issue may affect your patients.5,6,7,8
Pre-Curved Perimodiolar Arrays vs. Lateral Wall Arrays
First, let’s look at the basic design differences between pre-curved perimodiolar arrays and flexible lateral wall arrays.
Pre-curved perimodiolar electrode arrays are designed to wrap around the modiolus of the cochlea.
- Pre-curved spring array design
- One size only
- Pointed electrode array tip9
- Electrode array coils against modiolus9
- Stiff wire stylet used for insertion9
- Scala tympani placement uncertain1,2,3,4,9
- Deviation into scala vestibuli common1,2,3,4,9
- Tip fold-over rate of up to 8% 5,6,7,8
Flexible lateral wall electrode arrays are designed to freely conform to the curve of each cochlea. All MED-EL arrays are flexible lateral wall arrays—and only MED-EL offers truly flexible lateral wall arrays.
- Free-fitting straight array design9
- Wide range of array lengths for best fit9
- Rounded electrode array tip9
- Adapts to curve of scala tympani9
- Insertion without stylet9
- Reliable scala tympani placement3,9,10
- Ideal for structure preservation9,10
- Fold-over practically impossible (≤.005%)11
MED-EL cochlear implants have always used highly flexible lateral wall arrays. These arrays provide superior atraumaticity and minimal insertion force through wave-shaped wires, optimal contact spacing, and ultra-soft FLEX-Tip technology. These key design features are what set MED-EL flexible lateral wall arrays apart from pre-curved perimodiolar arrays and other lateral wall arrays.
Wave-Shaped Wires
In fact, MED-EL arrays are the only electrode arrays to feature wave-shaped wires distributed evenly throughout the electrode array. This makes our arrays incredibly flexible in every direction. This superior flexibility is only possible because every one of our arrays is handcrafted by an expert technician.
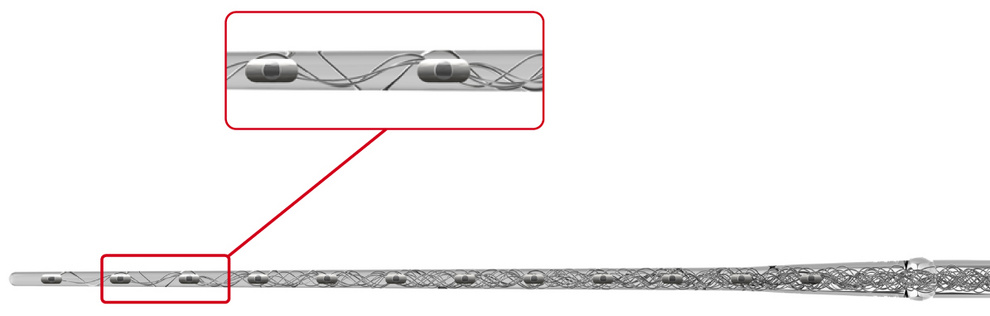
The wave-shaped wires in MED-EL arrays provide exceptional flexibility in all directions. The wires are distributed evenly throughout the electrode array.
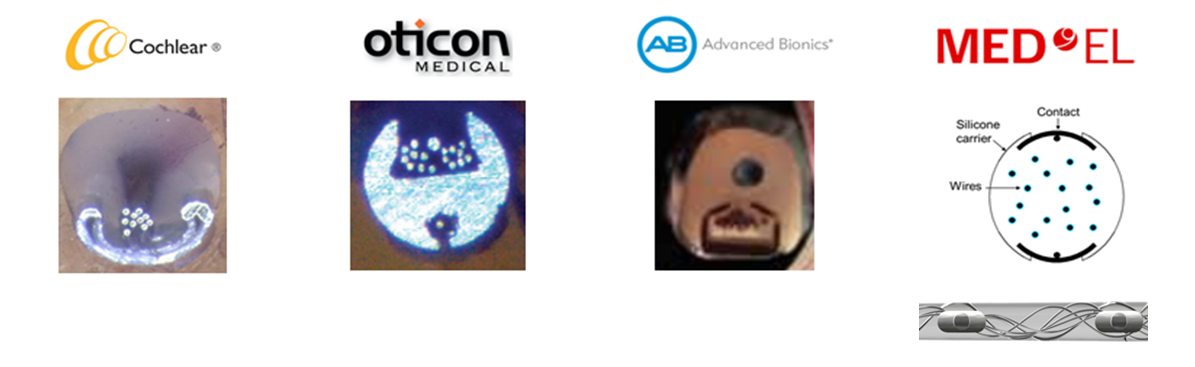 Other companies use straight wires densely bundled together—which makes these other electrodes arrays far stiffer and can lead to increased insertion force.9
Other companies use straight wires densely bundled together—which makes these other electrodes arrays far stiffer and can lead to increased insertion force.9
Electrode Array Tip
Another significant difference in design is the tip of the array, especially its shape. During insertion, the electrode array tip is the leading edge that guides the placement of the electrode array. Inside the cochlea, the lateral wall is fairly smooth, but the wall of the modiolus is a highly porous surface.9,12
That’s why MED-EL arrays use a rounded tip that gently deflects to guide the array to the most suitable placement. In contrast, pre-curved arrays such as the Cochlear™ Contour Advance® or Cochlear™ CI532 Slim Modiolar electrode use a pointed tip.
Let’s look at why design makes all the difference during electrode array insertion.
Atraumatic Electrode Insertion
During any electrode insertion, the array must travel from the site of insertion to the final position. Ideally, the array would be inserted through the round window and remain fully in the scala tympani as it travels toward the apex of the cochlea.
With flexible MED-EL lateral wall arrays, the rounded FLEX-Tip design gently deflects away from delicate structures, including the basilar membrane and spiral ligament. This free-fitting array design offers reliable scala tympani insertion for a wide variety of cochlear anatomies and with the lowest reported risk of tip fold-over.1,2,3,9,10,11,13-22
Flexible MED-EL electrode arrays can freely adapt to fit the unique shape of each individual cochlea.
Pre-curved Perimodiolar Electrode Tip Fold-Over
In contrast, when a pre-curved array is inserted, the array tip is continuously curving inward toward the center of the cochlea. If this pointed array tip is in contact with the highly porous modiolar wall or other intra-cochlear structure, the electrode array tip may catch and become lodged.5,6,7,8
Once the pre-curved perimodiolar array tip becomes lodged, several outcomes are possible. Often, pre-curved perimodiolar arrays can puncture the basilar membrane and deviate from the scala tympani to the scala vestibuli. This can result in significantly lower speech perception scores and loss of any residual hearing.1,2,3,4
However, there’s another issue that can occur when the pre-curved perimodiolar array tip becomes lodged or meets resistance—often referred to as electrode array tip fold-over or tip rollover. Basically, in tip fold-over or tip rollover, the electrode array folds over upon itself. The array tip can bend back towards the insertion point or laterally through cochlear structures.
Graphical representation of tip fold-over with pre-curved perimodiolar electrode array.8
Tip Fold-Over Complications
Clearly, an electrode array folded over upon itself is not a desired outcome. Often, the folded electrode deviates out of the scala tympani, causing damage to the cochlea.5,6,7,8 For your patients, this can mean significantly lower speech performance.
Of course, tip fold-over would also make an already short array even shorter—which could seriously limit the effective stimulation range of the array. A folded tip can result in less than half a turn of coverage in the cochlea. This would result in even worse place-pitch mismatch, which can have a serious impact on hearing performance.
Complications can include: 5,6,7,8
- Vertigo
- Overlapping electrodes
- Reduced insertion depth
- Revision surgery or electrode reinsertion
- Deviation into the scala vestibuli
- Deactivation of multiple electrodes
- Limited mapping potential
- Distorted sound quality
- Poor hearing performance
- Reduced overall benefit from CI
It’s important to note that tip fold-over may not be noticeable during implantation. Intraoperative neural response telemetry may not effectively identify tip fold-over. Additional intraoperative CT imaging and neural response telemetry could be necessary to confirm tip fold-over. If the fold-over is detected intraoperatively, reinsertion of the electrode during surgery may correct the fold-over, but this also adds further risk of trauma to the cochlea.5,6,7,8
If the tip fold-over is not identified intra-operatively, reimplantation surgery may be necessary. Otherwise, multiple electrodes may likely be deactivated during fitting—which can reduce overall patient benefit from the CI.5,6,7,8,15
Avoiding Tip Fold-Over
Electrode array tip fold-over is a complication that should be avoided in every case. It can result in sub-par electrode placement, reduced speech perception, and additional challenges for audiologists. Yet it remains a surprisingly common risk with pre-curved perimodiolar electrode arrays. 5,6,7,8
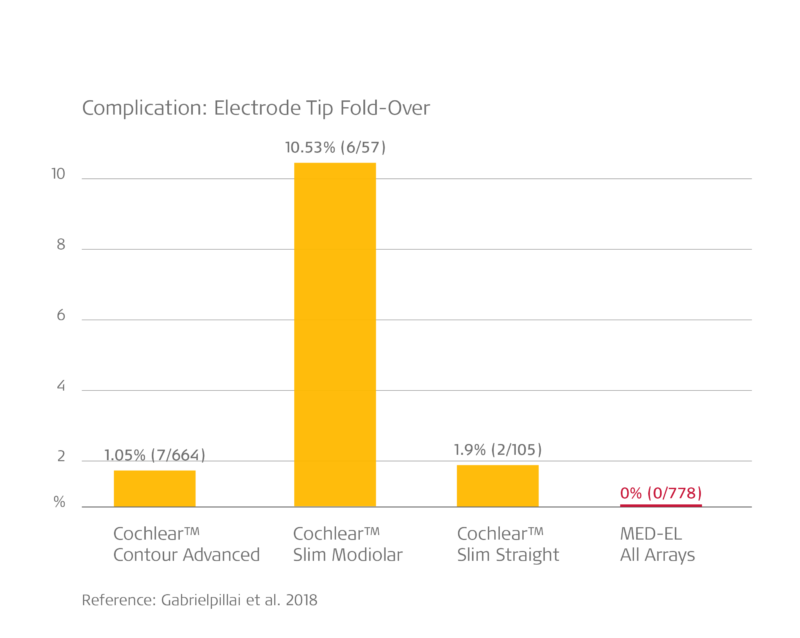
In Gabrielpillai et al. (2018), experienced surgeons encountered a tip fold-over rate of more than 10% of Slim Modiolar CI532 arrays. In contrast, 778 flexible MED-EL arrays were implanted—post-operative imaging confirmed that there were no cases of tip fold-over. Contour AdvanceTM and Slim Straight arrays also folded over in multiple cases, though less frequently.1
Atraumatic lateral wall arrays from MED-EL offer reliable scala tympani placement and the lowest reported rate of tip fold-over.13-22 With MED-EL, your patients can benefit from better hearing performance and more natural sound quality.
Get in Touch
Want to know more about MED-EL implants for your clinic? Contact your local MED-EL representative to get started.
References
- O’Connell, B.P., Hunter, J.B., & Wanna, G.B., (2016). The importance of electrode location in cochlear implantation. Laryngoscope Investigative Otolaryngology, 1: 169–174.
- Wanna, G.B., Noble, J.H., Carlson, M.L., Gifford, R.H., Dietrich, M.S., Haynes, D.S., Dawant, B.M., & Labadie, R.F. (2014). Impact of electrode design and surgical approach on scalar location and cochlear implant outcomes. Laryngoscope. 124(6):1–7.
- O’Connell, B.P., Cakir, A., Hunter, J.B., Francis, D.O., Noble, J.H., Labadie, R.F., Zuniga, G., Dawant, B.M., Rivas, A., & Wanna, G.B. (2016). Electrode location and angular insertion depth are predictors of audiologic outcomes in cochlear implantation. Otol Neurotol. 37(8):1016–1023.
- Boyer, E., Karkas, A., Attye, A., Lefournier, V., Escude, B., & Schmerber, S. (2015) Scalar localization by cone-beam computed tomography of cochlear implant carriers: A comparative study between straight and periomodiolar precurved electrode arrays. Otol Neurotol. 36(3):422–429.
- Zuniga, M.G., Rivas, A., Hedley-Williams, A., Gifford, R.H., Dwyer, R., Dawant, B.M., Sunderhaus, L.W., Hovis, K.L., Wanna, G.B., Noble, J.H., & Labadie, R.F. (2016) Tip fold-over in cochlear implantation: Case series. Otol Neurotol. 38(2):199–206.
- Cosetti, M.K., Troob, S.H., Latzman, J.M., Shapiro, W.H., Roland, J.T. Jr., & Waltzman, S.B. (2012) An evidence-based algorithm for intraoperative monitoring during cochlear implantation. Otol Neurotol. 33: 169–176.
- Grolman W, Maat A, Verdam F, et al. (2009) Spread of excitation measurements for the detection of electrode array fold-overs: A prospective study comparing 3-dimensional rotational x-ray and intraoperative spread of excitation measurements. Otol Neurotol 30:27–33.
- McJunkin, J.,L., Durakovic, N., Herzog, J., & Buchman, C.,A. (2018) Early Outcomes With a Slim, Modiolar Cochlear Implant Electrode Array. Otol Neurotol. 39(1):e28-e33.
- Dhanasingh, A. & Jolly, C. (2017) An overview of cochlear implant electrode array designs. Hear Res.356: 93–103.
- Nordfalk, K., Rasmussen, K., Hopp, E., Bunne, M., Silvola, J.T., & Jablonski, G.E., (2016). Insertion Depth in Cochlear Implantation and Outcome in Residual Hearing and Vestibular Function. Ear Hear. 37(2):e129–137.
- Data on file. Based on internal database dating back to 1996.
- Chole, R. (2015) Endoscopic view of the Scala Tympani. Otology & Neurotology. 36 (3):e97–e98
- Aschendorff, A., Briggs, R., Brademann, G., Helbig, S., Hornung, J., Lenarz, T., Marx, M., Ramos, A., Stoever, T., Escude, B., & James, C.J. (2017). Clinical investigation of the Nucleus Slim Modiolar Electrode. Audiol Neurootol. 22(3). 169–179
- Friedmann, D.R., Kamen, E., Choudhury, B., & Roland, J.T. (2019). Surgical experience and early outcomes with a slim perimodiolar electrode. Otol Neurotol. 40(3).
- Gabrielpillai, J., Burck, I., Baumann, U., Stoever, T., Helbig, S. (2018). Incidence for Tip Foldover During Cochlear Implantation. Otology Neurotology, 39(9): 1115–1121.
- Gomez Serrano, M., Patel, S., Harris, R., & Selvadurai, D. (2019).
Initial surgical and clinical experience with the Nucleus CI532 slim modiolar electrode in the UK. Cochlear Implants Int. 20(4).207–216. - Jia, H., Torres, R., Nguyen, Y., De Seta, D., Ferrary, E., Wu, H., Sterkers, O., Bernardschi, D., & Mosnier, I. (2018). Intraoperative conebeam CT for assessment of intracochlear positioning of electrode arrays in adult recipients of cochlear implants. AJNR Am J Neuroradiol. 39(4). 768–774.
- Lohmann, A.R., Carlson, M.L., & Sladen, D.P. (2018). Intraoperative cochlear implant device testing utilizing an automated remote system: A prospective pilot study. Otol Neurotol. 39(3). 313–317.
- Sipari, S., Iso-Mustajarvi, M., Lopponen, H., & Dietz, A. (2018). The insertion results of a Mid-Scala electrode assessed by MRI and CBCT image fusion. Otol Neurotol. 39(10).
- Stefanescu, E.H. & Motoi, S. (2018). Selection of the appropriate cochlear electrode array using a specifically developed research software application. J Laryngol Otol. 132(6). 544–549.
- Timm, M.E., Majdani, O., Weller, T., Windeler, M., Lenarz, T., Buechner, A. & Salcher, R.B. (2018). Patient specific selection of lateral wall cochlear implant electrodes based on anatomical indication ranges. PLoS ONE 13(10).
- Mittmann, P., Lauer, G., Ernst, A., Mutze, S., Hassepass, F., Arndt, S., Arweiler-Harbeck, D., & Christov, F. (2020). Electrophysiological detection of electrode fold over in perimodiolar cochlear implant electrode arrays: a multi center study case series. Eur Arch Otorhinolaryngol. 277(1). 31–35.
*Not all products, indications, and features shown are available in all areas. Please contact your local MED-EL representative for more information.
MED-EL



Was this article helpful?
Thanks for your feedback.
Sign up for newsletter below for more.
Thanks for your feedback.
Please leave your message below.
CTA Form Success Message
Send us a message
Field is required
John Doe
Field is required
name@mail.com
Field is required
What do you think?
The content on this website is for general informational purposes only and should not be taken as medical advice. Please contact your doctor or hearing specialist to learn what type of hearing solution is suitable for your specific needs. Not all products, features, or indications shown are approved in all countries.
MED-EL