

Join Clinicians Worldwide
Evidence-based insights to enhance hearing care—twice a month
Subscribe Now Evidence-based insights to enhance hearing care—twice a month
Subscribe NowMED-EL
Published Nov 23, 2018

MRI is an essential imaging modality, which is why we design all of our hearing implants for safe, comfortable access to MRI. This allows patients & clinicians to perform routine MRI scans without needing to surgically remove the implant magnet.
However, due to magnetic elements in the implant, image artifacts or shadowing can be present. When performing an MRI scan in patients with an hearing implant, usually an artifact is visible in the head region directly around the implant site.
Other regions are not generally affected—so a knee scan, back scan, or even neck scan should not be an issue. Even a head scan is not wholly affected; clear imaging of the contralateral region is possible. Imaging artifact also depends on the type of implant and the scanning parameters.
When scanning a BONEBRIDGE user, for example, there can be an significant image artefact, which can be a challenge if you want to examine ipsilateral head regions, such as the internal auditory canal.
To reduce the issues of imaging artifacts, many scanners offer “metal artifact reducing sequences” (MARS) which can be selected in the software of the MRI scanner. These sequences can reduce the size of the artefact considerably.
Today, we have a special interview with the ENT surgeons Prof. Dr. Javier Gavilán, Prof. Dr. Luis Lassaletta, M.D., and the neuroradiologists Dr. Cristina Utrilla, M.D., PhD, and Dr. Pilar García Raya, M.D, from the University Hospital La Paz in Madrid, Spain. They have extensive experience in implanting and scanning hearing implants and we are very happy that they are sharing their insights with us today.
Welcome, Prof. Gavilán, Prof. Lassaletta, Dr. Utrilla and Dr. García Raya!
MRI is a very important diagnostic tool. How do you evaluate the advantages of MRI?
C. Utrilla & P. García Raya: MRI is one of the imaging techniques that have experienced a great advance in recent years. The technical development is marked not only by the improvement and optimization of conventional MR imaging techniques but also by the emergence of new pulse sequences such as those with metal artifact reduction. Advances in physics, informatics and technology allow performing MRI studies in cases that several years ago were unimaginable; and patients with hearing implants are an example.
Is MRI the preferred diagnostic tool in your clinic?
L. Lassaletta: MRI is widely used in our clinic for multiple indications. Most people will undergo at least one MRI during life. In otologic patients, both CT and MRI are usually performed.
C. Utrilla & P. García Raya: We use both, CT and MRI, in patients using implants depending on the indication of the study. In general, we use CT in presurgical planning and in cases that a complication is suspected. MRI is useful in presurgical planning and for the follow up of the disease, for example in patients with neurofibromatosis type II, and to rule out other CNS pathologies.
J. Gavilán: MRI is crucial for the diagnosis and treatment plan of patients with hearing disorders. I would not say it is the preferred diagnostic tool because I do not think there is a “preferred” diagnostic tool. But it provides a crucial part of the information required for a correct diagnosis and an adequate treatment.
Not every MRI scanner offers metal artifact reducing sequences by default. However, the feature may be obtained with a software update or upgrade. With which MRI machine do you work?
C. Utrilla. & P. García Raya: In our institution we have 4 MRI scanners, one Philips High Field Open (Panorama®), one 1.5T Siemens (Avanto®), one 3T Siemens (Skyra®) and 1.5T General Electrics (Signa®). We use General Electrics Magnet to study patients with hearing implants.
The MARS sequence in GE (General Electrics) is known as MAVRIC (multiacquisition variable-resonance image combination). MAVRIC is an acquisition and reconstruction technique for imaging structures near to MR Conditional metallic devices; due to its characteristics it allows artifact reduction. Metal artifact–reduction techniques are designed to handle field inhomogeneity near large metallic implants of varying magnetic susceptibility.
Do you use the MAR sequences which are pre-set, or do you change the parameters?
C. Utrilla & P. García Raya: As this sequence is recommended for the study of joints after a prosthesis implant, we change the field of view to adjust to the region of interest, in this case, the head.
We also modified the slice thickness, in the MAVRIC sequence for musculoskeletal imaging they use 4 mm and for the head we select 3mm for the slice thickness.
For 3D sequences we can also select the locs per slab, it refers to the total number of slices generated from the slab, but the outermost 2 slices on each side are discarded (to deal with signal fading at the edges due to imperfect slab selection), in our case we use 48, against the 24 that are used for the musculoskeletal sequence.
From a surgical perspective: When implanting a BCI 601, which measures can be taken to influence the clarity of an MRI scan?
J. Gavilán: According to our current knowledge, the surgical position of the BC-FMT influences the quality of the MRI images. The position of the coil will also have an impact on the images, but this will be related to the surgical position of the BC-FMT and cannot be largely modified once the implant is in its final position.
L. Lassaletta: When implanting a patient who might need a cranial MRI (e.g. control of vestibular schwannoma), the further from the EAC (external auditory canal) you place the BC-FMT, the smaller the artifact will be. Middle fossa implantation may reduce the artifact when compared to retrosigmoid, and of course to mastoid implantation. On the other hand, placing the BC-FMT too far away from the cochlea (EAC) might affect hearing outcome and that should also be considered.
How many of your BONEBRIDGE patients did already have to undergo an MRI? What is more frequently needed—head or body MRI?
L. Lassaletta: As far as I recall, only one BB patient has undergone a head MRI. In the early days we were consulted for every MRI in patients with any implants. The radiologists are getting more used to it, so now it happens just sometimes.
J. Gavilán: Since one of our main indications for BB is patients with acoustic tumors, MRI is frequently required for their follow-up. Apart from this, most persons will need an MRI in their lifetime. This includes MRI for any medical condition affecting any part of the body. Therefore, MRI compatibility is a must in hearing implants.
Every time that a previously operated patient needs MRI we are asked about the implications of the imaging study on his or her previous operation.
Did you ever have a patient in whom a diagnosis initially was not possible but thanks to MARS it was?
C. Utrilla & P. García Raya: Indeed, we have a patient who suffers from epilepsy due to a cortical malformation (polymicrogyria). MRI was performed after a middle ear implant was placed and in the single sequence that we found that the polymicrogyria was bilateral was in the MAVRIC.
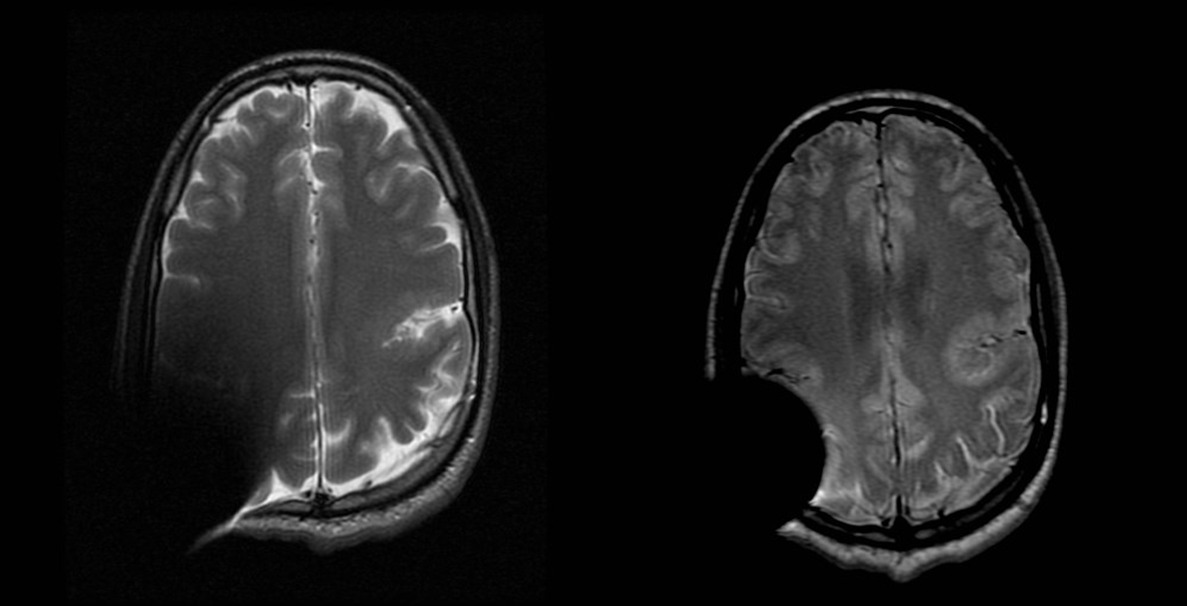
Left: Axial T2 left silvian fissure polymicrogyria in patient with a middle ear implant. Right: Axial PD MAVRIC showing bilateral silvian fissure polymicrogyria in patient with a middle ear implant.
By how many percent can the artifact of the BONEBRIDGE be reduced when MARS are used?
C. Utrilla & P. García Raya: We value the artifact surrounding the implant both quantitative and qualitative.
We calculate the radius measured from the geometrical center of the implant to the limit where we can evaluate the cerebral parenchyma. In our cases the artifact was reduced approximately 20 to 25%.
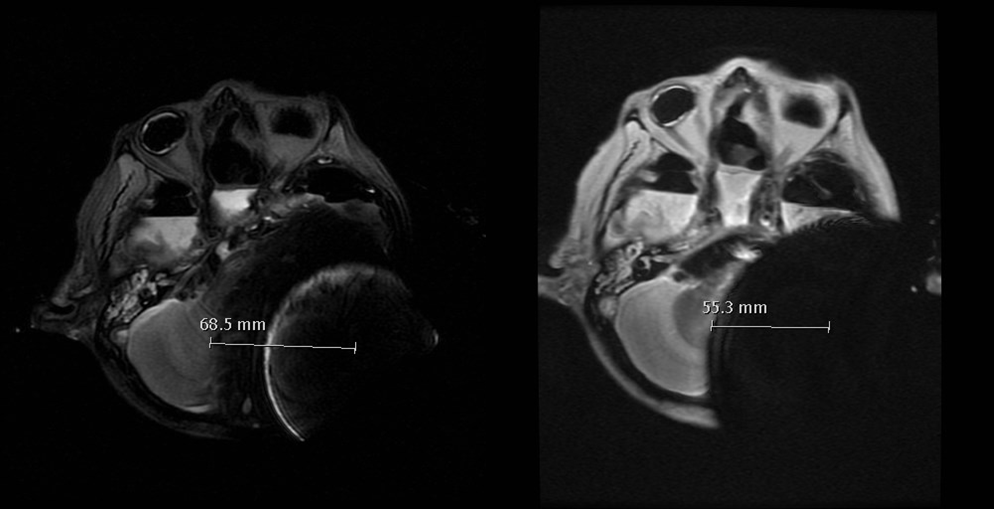
Left: BCI 601 using sinodural placement using a standard axial T2 SE sequence; Right: BCI 601 using sinodural placement with artifact removal sequence (axial MAVRIC).
On the other hand, for qualitative image analysis, we compared the anatomic resolution for the visualization of the brain, the pontocerebellar angle, and internal auditory canal adjacent to the artifact, with standard sequences and artifact reduction sequences. We can appreciate that the limits of the artifact produced by the implant are better defined in the metal artifact reduction sequences than in the standard long TE sequences.
Can you tell us something about the cadaver tests that you did with the BCI 601?
J. Gavilán: To assess the impact of the surgical position of the device, we implanted BB in cadaver heads using different anatomical sites. After implantation the heads were taken to MRI were images were obtained. The results from different locations were compared to assess their impact on the visibility of the surrounding structures.
C. Utrilla & P. García Raya:
We also compare the artifact depending on the location of the implant: using sinodural placement in one of the samples and the middle fossa approach on the other one.
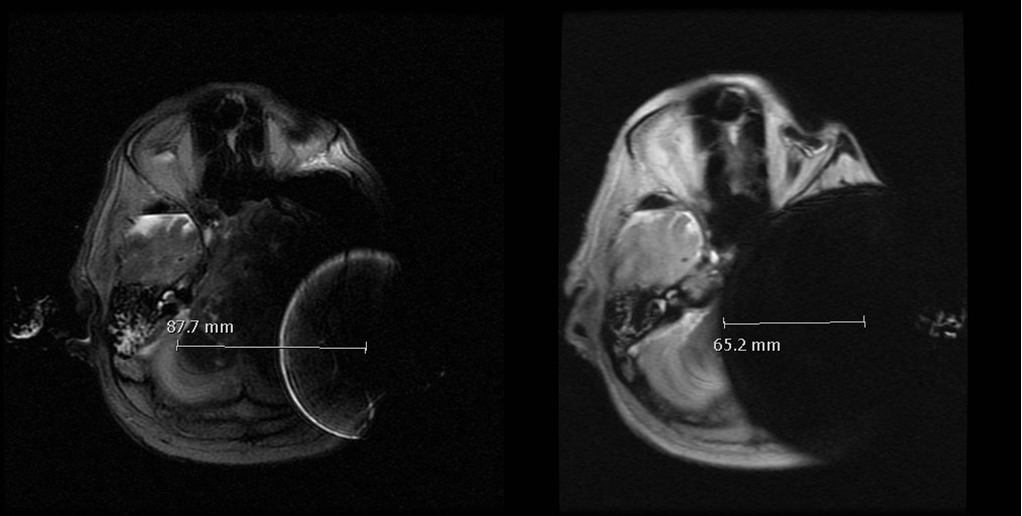
Left: BCI 601 using middle fossa placement, standard axial T2 SE sequence; Right: BCI 601 using middle fossa placement with artifact removal sequence (MAVRIC).
We conclude that artifact removal sequences, in addition to middle fossa approach, allow a better visualization of the posterior fossa, especially of the contralateral internal auditory canal.
Thank you Prof. Gavilán, Prof. Lassaletta, Dr. Utrilla and Dr. García Raya!
Want to learn more about MRI and MED-EL hearing implants? Find out how all of our hearing implants are made for easyMRI.
See all the MRI conditions for BONEBRIDGE and SOUNDBRIDGE here, and see MRI conditions for MED-EL cochlear implants here.
Don’t forget to subscribe to get all the latest articles sent right to your inbox!
*Not all products, features, and indications shown are available in all areas. Please contact your local MED-EL representative for more information.
MED-EL
Was this article helpful?
Thanks for your feedback.
Sign up for newsletter below for more.
Thanks for your feedback.
Please leave your message below.
CTA Form Success Message
Send us a message
Field is required
John Doe
Field is required
name@mail.com
Field is required
What do you think?
The content on this website is for general informational purposes only and should not be taken as medical advice. Please contact your doctor or hearing specialist to learn what type of hearing solution is suitable for your specific needs. Not all products, features, or indications shown are approved in all countries.
MED-EL
Get the latest research and resources to help people with every kind of hearing loss. Subscribe to the MED-EL Professionals Blog now.
Registration was successful
We’re the world’s leading hearing implant company, on a mission to help people with hearing loss experience the joy of sound.
Find your local MED-EL team
The content on this website is for general informational purposes only and should not be taken as medical advice. Please contact your doctor or hearing specialist to learn what type of hearing solution is suitable for your specific needs. Not all products, features, or indications shown are approved in all countries.


