
Published Dec 13, 2017
Best Bimodal Hearing: MED-EL Cochlear Implants and Hearing Aids

For a person with hearing loss, it can take years to find the right hearing aid. There are endless variations of form, features, and fitting parameters. Of course, there’s also significant cost to changing to a new hearing aid.
For cochlear implant candidates, this is an especially important consideration. Many unilateral cochlear implant recipients will continue to use a hearing aid in their contralateral ear. For these bimodal users, finding the right hearing aid has likely been a lengthy process.
And even with the right hearing aid, changes to compression ratio or frequency response can significantly affect hearing performance. So, if a person finds their best hearing aid match and ideal mapping for their needs, why should they have to suddenly change to a different hearing aid to use a bimodal solution?
As an audiologist, you want your patients to have the best possible outcomes. That’s why MED-EL cochlear implants are designed to provide outstanding bimodal hearing performance that can work with every brand and style of hearing aid.
How is this possible? Our philosophy is to deliver the closest possible match to natural hearing, making our cochlear implants a perfect match for nearly any hearing aid.1 We’re not tied to any hearing aid brand, so you are free to choose the best hearing aid option for each individual patient.
Today, we’re going to take a detailed look at what makes MED-EL the best choice for bimodal hearing—for every cochlear implant candidate with any hearing aid.
Bonus: We hosted a CEU webinar on bimodal for audiologists! This educational webinar is available to Audiology Online members and is guided by our bimodal experts. CEU course credits are available!
Hearing Aid Compatibility
First, let’s look at why universal compatibility between a hearing aid and cochlear implant is so important for bimodal users.
As an audiologist, you’ve likely seen constant promotion of brand-specific solutions. At first, these solutions seem like a logical solution—the hearing aid features can be “matched” to the features of the cochlear implant audio processor. Both Advanced Bionics™ and Cochlear™ promote a brand-specific hearing aid as a bimodal solution.2,3
However, these brand-specific bimodal solutions rely on features that are only compatible with a very narrow range of hearing aids. That means a cochlear implant candidate could be tied to a single brand for the life of their implant.
So, are there any exclusive benefits to having a system with these “shared features”?
The simple answer: No. There are no real practical benefits to these exclusive bimodal solutions that MED-EL cannot easily match. And what’s more important—MED-EL offers many advantages that these other systems cannot match.
Advanced Bionics™ & Naída™ Link2
- Similar front-end processing to brand-specific hearing aids
- Bimodal streaming
Cochlear™ & GN ReSound™3
- Bimodal streaming
- Requires two separate apps
- Requires two separate remotes
MED-EL
- Similar front-end processing to most hearing aids
- Bimodal streaming
- Hearing aid can be fitted independently to achieve the best benefit for the non-implanted ear
- Universal compatibility
- No additional cost
- Better music enjoyment4,5,6,7
- Better speech perception in noise8
- Most natural sound quality1
Compression Ratio
Advanced Bionics promotes their Naída bimodal solution as “the first hearing aid specifically designed to work with a cochlear implant system”.2 A less euphemistic version of this would point out that the hearing aid is being compromised to reduce the significant mismatch between the sound coding of an Advanced Bionics cochlear implant and the hearing aid.9
The Advanced Bionics Naída cochlear implant has a 12:1 compression ratio for automatic gain control. This is a serious mismatch to the approximately 2:1 compression ratio of hearing aid AGCs. Without similar compression ratios, loudness growth will be completely skewed between each ear. Such a mismatched AGC can cause significantly reduced hearing performance.9,10
Essentially, the hearing aid front-end processing is matched to the audio processor because it needs to be. This matching isn’t an exclusive benefit—it’s an exclusive necessity. Without a heavily modified compression ratio, users may experience significantly reduced hearing performance.9,10
Natural Loudness Growth
This high compression ratio isn’t an issue with MED-EL cochlear implant systems. Our dual-loop automatic gain control is designed to provide a loudness growth that’s much closer to natural hearing. Our standard AGC compression ratio is 3:1, which is closer to hearing aids, and can easily be adjusted.
This allows a natural loudness growth match between each ear, so your patients can hear soft sounds more easily and loud sounds more comfortably. This makes it easy to pair a MED-EL cochlear implant to nearly any hearing aid—a routine loudness balancing is generally the only bimodal fitting step necessary.
For bimodal MED-EL recipients, you can simply program the hearing aid to independently provide the best benefit to the non-implanted ear. This can help simplify fitting and logistics in your clinic.
Bimodal Streaming
Connectivity can be an important consideration for many candidates. They want to be able to stream audio from their phones, tablets, televisions, and more. That’s why we have a full range of bimodal streaming options. Our bimodal connectivity options are easy-to-use, affordable, and widely compatible with hearing aids.
Bluetooth neckloops enable bimodal streaming to our audio processors and any telecoil-compatible hearing aid. These Bluetooth neckloops offer broad compatibility with mobile phones, so recipients aren’t limited to one specific brand of phone.
For bimodal wireless streaming from a remote microphone, MED-EL recipients can use a wide range of wireless receivers that are designed to work with hearing aids, such as Oticon™ and Phonak™ wireless systems.11,12 This includes seamless connectivity to Roger™ wireless microphones from Phonak.
Natural Frequency Matching
So, it’s clear that MED-EL can easily match the bimodal features offered by Advanced Bionics and Cochlear. And, with MED-EL cochlear implants, these benefits aren’t limited to a specific line of hearing aids. Now, let’s look at how MED-EL bimodal solutions offer many advantages that every other bimodal hearing system cannot match.
A hearing aid generally provides a natural range of sound frequencies—approximately 100Hz through 8,000 Hz. This wide natural frequency range in important, as the low frequencies help provide a richer sound quality, and the higher frequencies are necessary for speech understanding.
In bimodal hearing, there are generally two methods of providing this range of low-to-high frequencies.13
- Complementary integration: Frequency spectrum is split between each ear
- Redundant integration: Broad spectrum sound to delivered to both ears
So, what determines if bimodal hearing is primarily complementary or redundant between ears? That’s where electrode array length and tonotopic coding come into play.
Tonotopic Coding
The cochlea is tonotopically arranged, with high frequencies coded in the basal turn and low pitches perceived deeper in the apical region. Only a long electrode array can reliably reach the lower-frequency regions towards the apex.14,15,16,17

MED-EL cochlear implants utilize long electrode arrays, enabling a natural place-pitch match from approximately 8,000 Hz down to 100 Hz. This allows a much more natural perception of a wide frequency range.14,15,16
With other companies, this natural place-pitch match is not possible. Short electrode arrays—such as perimodiolar or mid-scala arrays—cannot reach deep enough into the cochlea to offer natural perception of low frequencies.14,15,16,17
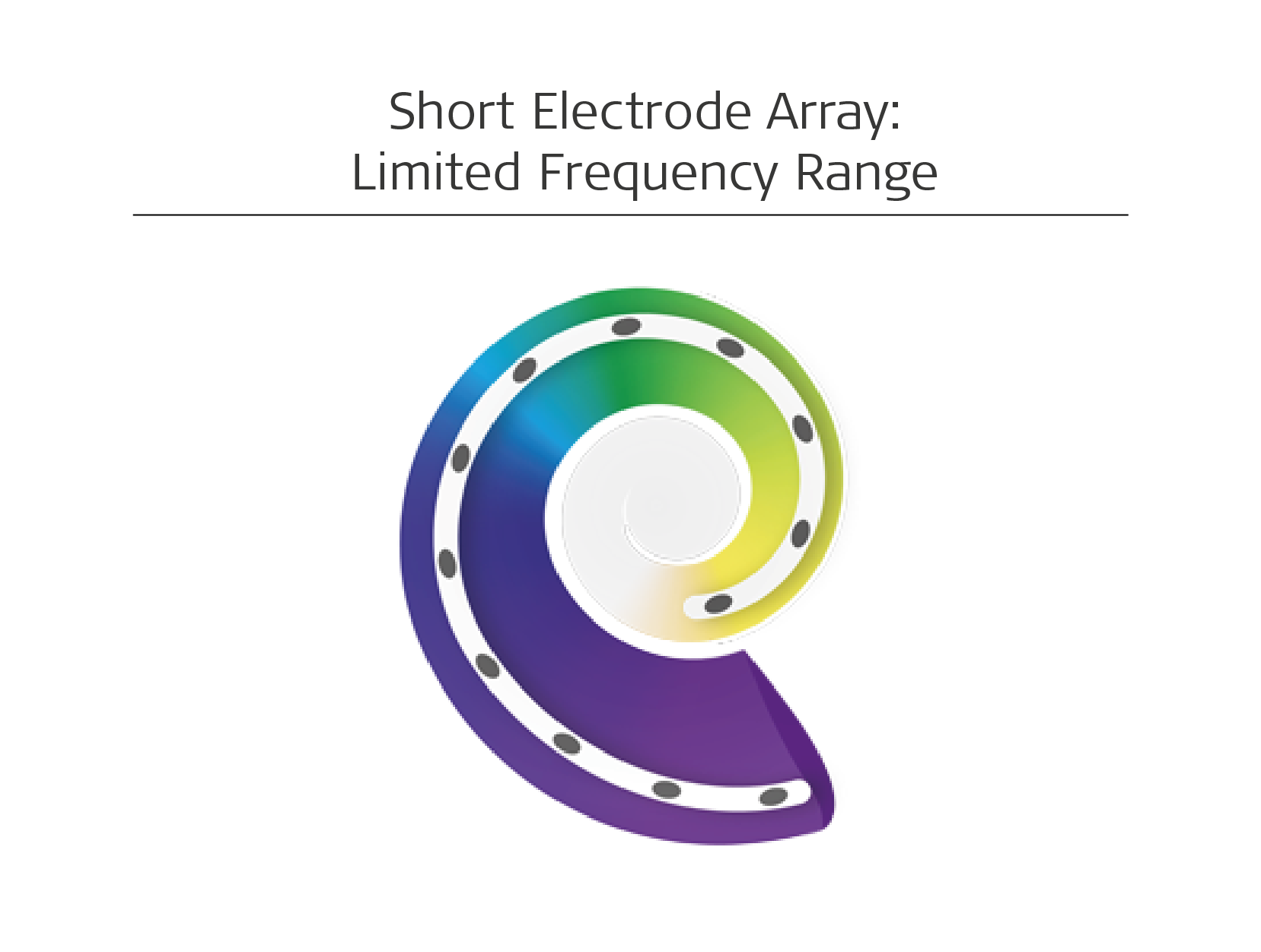
With these short electrode arrays, even the most apical electrode may likely only reach roughly the 600–800 Hz position on the natural tonotopic map. If an electrode array can’t reach the apical region in the second turn, low-to-mid pitches cannot be naturally mapped. You can’t rely on neural adaption to correct this mismatch—even partial correction can take years of use.14,15,16,17
Attempting to map lower frequencies into shallower portions of the cochlea would very likely result in significant pitch mismatch between the hearing aid and the cochlear implant.14,15,16,17 This lack of low-frequency information is why both Cochlear™ and Advanced Bionics bimodal solutions use a hearing aid to provide the low frequencies through complementary integration.18,19
Complementary Integration
Complementary integration relies on a hearing aid providing the low pitches in one ear and a cochlear implant providing the higher pitches in the other ear.13
- Hearing aid: Low frequencies (~100–750Hz)
- Cochlear implant: Mid-to-high frequencies (~750–8000Hz)
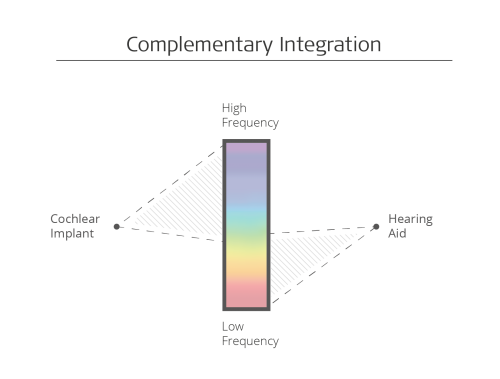
The goal with this concept is to provide speech understanding from the cochlear implant, and “richness” or “depth” from the low frequencies of the hearing aid. Only a limited range of the sound signal reaches each ear, so complementary integration may require additional central auditory processing to sort out the information.18,19,20
It’s important to note that a complementary strategy may require you refit the hearing aids to shift the frequency response curve toward the lower frequencies.9
For bimodal users who are happy with their current hearing aid program, shifting the frequency response curve or other fitting parameters could be unsatisfactory. Hearing aids are generally not fit to exaggerate the low frequencies. This means you may have to fit the hearing aid in a manner that reduces hearing performance in that ear.9
Redundant Integration
In contrast, when you offer a wider, more natural frequency range to both ears, a patient can benefit from redundant integration. This provides a more complete sound input to both ears, which can provide more robust and complete information to the brain from each ear.20
With a redundant strategy, the cochlear implant and the hearing aid are both fitted to independently provide a natural range of sounds from approximately 100Hz–8,000 Hz. That way, both ears have a wide overlap of matching frequency information.20
- Hearing aid: Low, mid, and high frequencies (~100Hz–8,000 Hz)
- Cochlear implant: Low, mid, and high frequencies (~100–8,000 Hz)
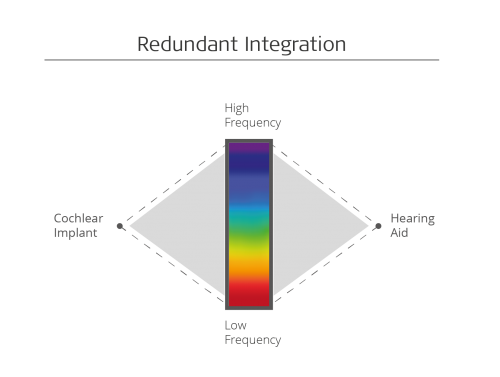
With long electrode arrays, MED-EL cochlear implants can offer wide-spectrum redundant integration for bimodal listeners.
This allows MED-EL cochlear implants to provide excellent speech understanding, while still having a natural pitch match to the hearing aid. This also allows the hearing aid to be independently fitted to provide best overall benefit to the non-implant ear, rather than only amplifying the low frequencies.
Even for patients with high-frequency hearing loss, redundant integration has key advantages. The cochlear implant can still provide useful redundant mid & low frequency information.
Redundant integration can provide true binaural hearing, and in general, when people hear with two ears, there are important benefits:
Binaural summation: Hearing with both ears provides a louder and more robust sound signal for the brain. This offers a 1–2 dB SNR improvement in noise for both normal-hearing and bilateral cochlear implant listeners, and can reduce listening effort in general.21,22,23,24,25
Squelch effect: By comparing sounds received in both ears, central auditory processing in the brain can improve the quality of a sound and filter out noise. This primarily uses redundant information of the sound as received by the two ears. Even an ear hearing mostly noise will still provide an SNR benefit of ~3 dB in normal-hearing listeners, as binaural listening provides a more complete sound signal for auditory processing.21,26
Interaural Time Differences (ITDs): If a sound source is not directly in front of the listener, it will reach the ears with a fraction of a second difference. These interaural time differences can provide localization cues for binaural listeners. Without accurate frequency and timing information from binaural low frequency hearing, this localization information can be lost.21,27
Interaural Level Differences (ILDs): Similar to ITDs, ILDs use a comparison of sound information between ears. As sound waves pass from one side of the head to the other, mid-to-high frequencies are blocked by the head. This creates a interaural level difference that can provide essential localization information. If a hearing aid only provides low frequencies or has a high AGC compression ratio, these localization cues can be lost.21,27
Best Bimodal Hearing Performance
So, what’s the key point you should take away from all this information?
For the best bimodal outcomes, pair the best cochlear implant with the right hearing aid for each candidate.
MED-EL cochlear implants offer superior hearing performance and the closest to natural hearing possible.1,8,28 This makes them the ideal match for every cochlear implant candidate with any hearing aid.
- More natural loudness growth
- Bimodal streaming
- Hearing aid independently fitted to best benefit
- Universal compatibility
- No additional cost
- Better music enjoyment4,5,6,7
- Better speech perception in noise8,28
- Most natural sound quality1,6,17
Share and Subscribe
Ready to take your professional knowledge on bimodal with MED-EL even further? Check out our CEU webinar on bimodal for audiologists! This educational webinar is available to Audiology Online members and is guided by our bimodal experts. CEU course credits are available!
*Not all products, indications, and features shown are available in all areas. Please contact your local MED-EL representative for more information.
References:
1. Rader, T., Döge, J., Adel, Y., Weissgerber, T., & Baumann, U. (2016). Place dependent stimulation rates improve pitch perception in cochlear implantees with single-sided deafness. Hear Res., 339, 94–103.
2. The Naída Bimodal Hearing Solution. https://www.advancedbionics.com/com/en/home/products/naida-bimodal-hearing-solution.html
3. Nucleus® 7 Sound Processor Bimodal Solution. http://www.cochlear.com/wps/wcm/connect/us/recipients/nucleus-7-bimodal-support
4. Müller, J., Brill, S., Hagen, R., Moeltner, A., Brockmeier, S.J., Stark, T., Helbig, S., Maurer, J., Zahnert, T., Zierhofer, C., Nopp, P., & Anderson, I. (2012). Clinical trial results with the MED-EL fine structure processing coding strategy in experienced cochlear implant users. ORL J Otorhinolaryngol Relat Spec., 74(4), 185–198.
5. Roy, A.T., Carver, C., Jiradejvong, P., & Limb, C.J. (2015). Musical sound quality in cochlear implant users: A comparison in bass frequency perception between Fine Structure Processing and High-Definition Continuous Interleaved Sampling Strategies. Ear Hear., 36(5), 582–590.
6. Roy, A.T., Penninger, R.T., Pearl, M.S., Wuerfel, W., Jiradejvong, P., Carver, C., Buechner, A., & Limb, C.J. (2016). Deeper cochlear implant electrode insertion angle improves detection of musical sound quality deterioration related to bass frequency removal. Otol Neurotol., 37(2), 146–151.
7. Prentiss, S.M., Friedland, D.R., Nash, J.J., & Runge, C.L. (2015). Differences in Perception of Musical Stimuli among Acoustic, Electric, and Combined Modality Listeners. J Am Acad Audiolol. 26(5):494–501.
8. Kleine Punte, A., De Bodt, M., & Van de Heyning, P. (2014). Long-term improvement of speech perception with the Fine Structure Processing coding strategy in cochlear implants. ORL, 76, 36–43.
9. Optimizing Hearing for Listeners with a Cochlear Implant and Contralateral Hearing Aid: Adaptive Phonak Digital Bimodal Fitting Formula. http://www.phonaknhs.co.uk/ProductDownloads/Upload/Bimodal_Fitting_Formula_White_Paper.pdf
10. Veugen, L.C., Chalupper, J., Snik, A.F., Opstal, A. J., & Mens, L.H. (2016). Matching automatic gain control across devices in bimodal cochlear implant users. Ear Hear. 37(3):260–270
11. Amigo FM System. https://www.oticon.com/solutions/for-children/amigo-fm
12. RogerTM Receivers. https://www.phonakpro.com/com/en/products/wireless-accessories/roger-receivers/overview-roger-receivers.html
13. Yoon, Y.S., Shin, Y.R., Gho, J.S., & Fu, Q.J. (2015). Bimodal benefit depends on the performance difference between a cochlear implant and a hearing aid. Cochlear Implants Int. 16(3):159–167.
14. Greenwood, D.D. (1990) A cochlear frequency-position function for several species–29 years later. J Acoust Soc Am., 87(6), 2592–2605.
15. Landsberger, D.M., Svrakic, M., Roland, J.T. Jr., & Svirsky, M. (2015). The relationship between insertion angles, default frequency allocations, and spiral ganglion place pitch in cochlear implants. Ear Hear., 36(5), 207–213.
16. Prentiss, S., Staecker, H., & Wolford, B. (2014). Ipsilateral acoustic electric pitch matching: a case study of cochlear implantation in an up-sloping hearing loss with preserved hearing across multiple frequencies. Cochlear Implants Int., 15(3), 161–165.
17. McDermott, H., Sucher, C., & Simpson, A. (2009) Electro-acoustic stimulation. Acoustic and electric pitch comparisons. Audiol Neurootol., 14(1), 2–7.
18. Bimodal Hearing: Cochlear Implants and Hearing Aids Together. http://www.cochlear.com/wps/wcm/connect/uk/for-professionals/sound-connection/bimodal-hearing
19. Help your patients hear their best in both ears – with Smart Bimodal Solutions. http://www.cochlear.com/wps/wcm/connect/us/for-professionals/products/cochlear-implants/smart-bimodal-solutions
20. Sheffield, S. Simha, M., Jahn, K., & Gifford, R. (2016) The effects of acoustic bandwidth on simulated bimodal benefit in children and adults with normal hearing. Ear Hear. 37(3): 282–288.
21. Mertens G; De Bodt M; Van de Heyning P (2017). Evaluation of Long-Term Cochlear Implant Use in Subjects With Acquired Unilateral Profound Hearing Loss: Focus on Binaural Auditory Outcomes. Ear Hear, 38(1), p. 117-125
22. Bronkhorst AW; Plomp R (1989). Binaural speech intelligibility in noise for hearing-impaired listeners. J Acoust Soc Am, 86(4), p. 1374-1383
23. Cox RM; DeChicchis AR; Wark DJ (1981). Demonstration of binaural advantage in audiometric test rooms. Ear Hear, 2(5), p. 194-201
24. Müller J; Schön F; Helms J (2002). Speech understanding in quiet and noise in bilateral users of the MED-EL COMBI 40/40+ cochlear implant system. Ear Hear, 23(3), p. 198-206
25. Schleich P; Nopp P; D’Haese P (2004). Head shadow, squelch, and summation effects in bilateral users of the MED-EL COMBI 40/40+ cochlear implant. Ear Hear, 25(3), p. 197-204
26. Bronkhorst AW; Plomp R (1988). The effect of head-induced interaural time and level differences on speech intelligibility in noise. J Acoust Soc Am, 83(4), p. 1508-1516
27. Shaw EA (1974). Transformation of sound pressure level from the free field to the eardrum in the horizontal plane. J Acoust Soc Am, 56(6), p. 1848-1861
28. Buchman, C.A., Dillon, M.T., King, E.R., Adunka, M.C., Adunka, O.F., & Pillsbury, H.C. (2014). Influence of cochlear implant insertion depth on performance: a prospective randomized trial. Otol Neurotol., 35(10), 1773–1779.



CTA Form Success Message
Send us a message
Field is required
John Doe
Field is required
name@mail.com
Field is required
What do you think?
The content on this website is for general informational purposes only and should not be taken as medical advice. Please contact your doctor or hearing specialist to learn what type of hearing solution is suitable for your specific needs. Not all products, features, or indications shown are approved in all countries.