

Published Jun 14, 2017
Why You Need Both Tonotopic and Temporal Fine Structure Coding
In the first part of this series on cochlear implant sound quality, we looked at electrode arrays. Specifically, we saw how long electrode arrays are necessary for place-pitch match in the mid-to-low frequencies. If an array can’t reach the second turn of the cochlea, it can’t provide natural tonotopic coding for lower frequencies.
Yet beyond the first turn, place-pitch match is only the first step. Now we’ll look at the second half of the equation—sound frequency-matched rate coding in the apical region.
Let’s take a look at why you need a sound coding strategy that provides both tonotopic (place) and temporal (rate) coding for the most accurate pitch perception.
Natural Rate Coding
With natural hearing, a more complex arrangement comes into play in the second turn of the cochlea. In addition to tonotopic coding, a form of rate coding appears. Here in the apical region, hair cells are able to trigger nerve signals in sync with the frequency of sound signals.1,2
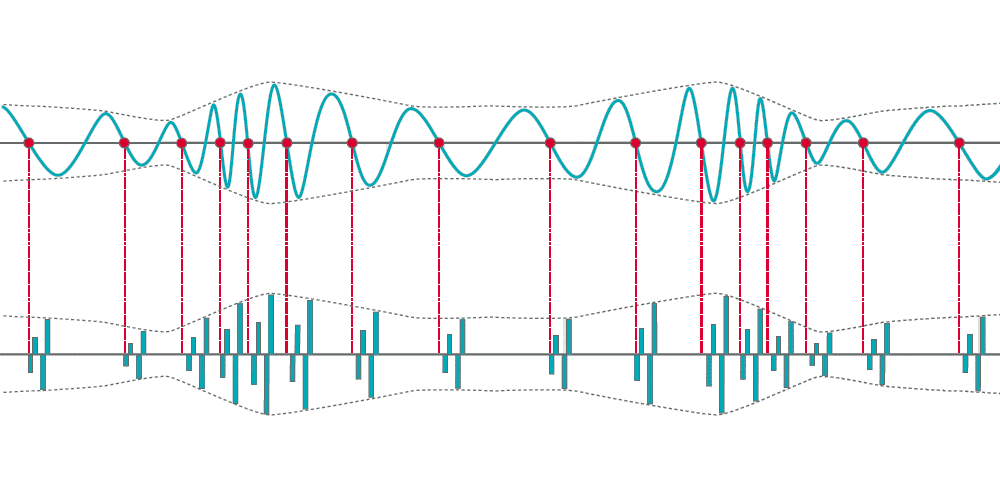
For mid-to-low frequencies, each cycle of a sound wave opens and closes a hair cell response—like turning a light switch on and off. Sound frequency is measured in cycles per second (Hz), so in theory, a 110 Hz sound wave triggers 110 compound action potentials per second in the auditory nerve fiber. A 263 Hz tone would trigger 263 compound action potentials per second, a 440 Hz tone would trigger 440 compound action potentials, and so on. This phase-locking synchronizes the action potentials to the incoming sound wave.2
This one-to-one rate coding enables precise natural frequency tuning that likely wouldn’t be possible with place coding alone. It’s often referred to as temporal coding, because it can provide the precise time coding of sound. Temporal coding is believed to have an important role in speech understanding in noise, pitch perception, music appreciation, and sound localization.1,2
At approximately 1,000 Hz, the firing rate of individual nerve fibers becomes increasingly saturated and tonotopic coding takes over. That’s why tonotopic coding and temporal coding are both essential in natural hearing.1,2
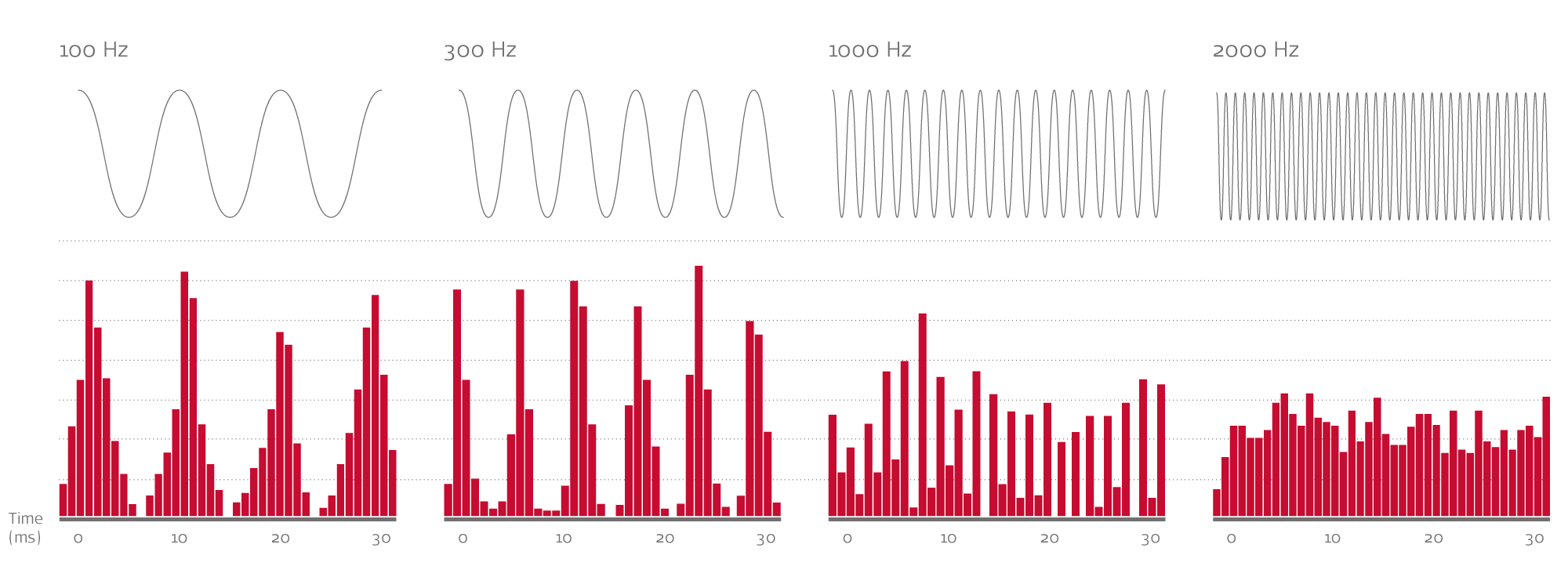 Phase-locked temporal coding in the auditory nerve can be seen up to roughly 1000 Hz, where the individual neural firing rate becomes saturated. Visual approximation of phase-locking; image for illustrative purposes only, based on Pickles, et al. (2013).
Phase-locked temporal coding in the auditory nerve can be seen up to roughly 1000 Hz, where the individual neural firing rate becomes saturated. Visual approximation of phase-locking; image for illustrative purposes only, based on Pickles, et al. (2013).
Rate Coding in Cochlear Implants
If a long array can provide place-pitch match in the second turn of the cochlea, why does rate coding matter for cochlear implant recipients?
Accurate rate coding in the second turn of the cochlea is essential for more natural perception of mid-to-low frequencies. If the implant uses a fixed rapid pulse rate (e.g. 1,500 pulses per second), it can distort pitch perception on electrodes in the apical region. A pulse rate that’s too high will cause pitch perception to shift upwards. 3,4,5
Think of it like playing a record on a turntable. At the right speed, the music sounds natural. But if you speed up the turntable, it shifts everything up in pitch. So, for accurate low-frequency perception, an implant needs to mimic natural rate coding in the second turn of the cochlea. This means slowing down pulse rate to match the sound frequency.3,4,5,6
Let’s look at recent pitch-matching experiments with recipients who had relatively normal hearing in their non-implanted ear, or even residual hearing in their implanted ear. These studies have shown rate-matched pulses on place-matched electrode—for example, 100 pps for a 100 Hz signal on an apical electrode in the second turn—can deliver accurate pitch perception down to approximately 100 Hz.3,4,6,7
These low frequencies are essential for a rich, full, resonant sound—without the low frequencies, sound quality can be “robotic”, “tinny”, “echoey”, or “mechanical”.8
However, rate coding isn’t effective in the first turn of the cochlea—a low pulse rate on a short array can’t effectively lower the pitch enough, and can produce an unpleasant or annoying sound quality.3,5,6 So if an electrode array can’t reach the apical region, it can’t mimic natural rate coding. This means low-to-mid pitches cannot be mapped according to the Greenwood function. Without access to accurate tonotopic or rate coding, natural perception of the lower frequencies is out of reach on short arrays.3,4,7,9,10
More Natural Sound Quality
There’s only one way to achieve more natural pitch perception across the whole cochlea—by combining long electrode arrays with precise, rate-matched stimulation.4,5,6,7
What benefits can long arrays and pitch-matched rate coding offer for your patients?
- Significantly better speech understanding in a short time frame 11,12
- More natural pitch perception 3,4,9
- Up to 250 spectral bands/virtual channels
- “Vocals much more clear and resonant” and “Deeper, more resonant, more natural sound” 8
- Better music appreciation and more natural perception of music 13,14,15
- Significantly better speech perception in quiet & noise 16
And lastly, “An unparalleled restoration of tonotopic pitch perception”—Rader et al. (2016)4
Have a question about long arrays and rate-matched sound coding? Leave a comment below!
We’ll be taking a closer look at sound coding in upcoming articles—subscribe now to make sure you don’t miss any posts!
*Not all products, indications, and features shown are available in all areas. Please contact your local MED-EL representative for more information.
References:
- Moon, I.J., & Hong, S.H. (2014). What is temporal fine structure and why is it important? Korean J Audiol., 18(1), 1–7.
- Pickles, J.O. (2013). An introduction to the physiology of hearing. 4th ed. Leiden, Netherlands: Koninklifke Brill NV.
- Schatzer, R., Vermeire, K., Visser, D., Krenmayr, A., Kals, M., Voormolen, M., Van de Heyning, P., & Zierhofer, C. (2014) Electric-acoustic pitch comparisons in single-sided-deaf cochlear implant users: frequency-place functions and rate pitch. Hear Res., 309, 26–35.
- Rader, T., Döge, J., Adel, Y., Weissgerber, T., & Baumann, U. (2016). Place dependent stimulation rates improve pitch perception in cochlear implantees with single-sided deafness. Hear Res., 339, 94–103.
- Landsberger, D.M., Vermeire, K., Claes, A., Van Rompaey, V., & Van de Heyning, P. (2016). Qualities of single electrode stimulation as a function of rate and place of stimulation with a cochlear implant. Ear Hear., 37(3), 149–159.
- Prentiss, S., Staecker, H., & Wolford, B. (2014). Ipsilateral acoustic electric pitch matching: a case study of cochlear implantation in an up-sloping hearing loss with preserved hearing across multiple frequencies. Cochlear Implants Int., 15(3), 161–165.
- Landsberger, D.M., Svrakic, M., Roland, J.T. Jr., & Svirsky, M. (2015). The relationship between insertion angles, default frequency allocations, and spiral ganglion place pitch in cochlear implants. Ear Hear., 36(5), 207–213.
- Harris, R.L., Gibson, W.P. Johnson, M., Brew, J., Bray, M., & Psarros, C. (2011) Intra-individual assessment of speech and music perception in cochlear implant users with contralateral Cochlear and MED-EL systems. Acta Otolaryngol., 131(12), 1270–1278.
- Vermeire, K., Landsberger, D.M., Van de Heyning, P., Voormolen, M., Kleine Punte, A., Schatzer, R., & Zierhofer, C.(2015) Frequency-place map for electrical stimulation in cochlear implants: Change over time. Hear Res., 326, 8–14.
- McDermott, H., Sucher, C., & Simpson, A. (2009) Electro-acoustic stimulation. Acoustic and electric pitch comparisons. Audiol Neurootol., 14(1), 2–7.
- Buchman, C.A., Dillon, M.T., King, E.R., Adunka, M.C., Adunka, O.F., & Pillsbury, H.C. (2014). Influence of cochlear implant insertion depth on performance: a prospective randomized trial. Otol Neurotol., 35(10), 1773–1779.
- Helbig, S., Helbig, M., Leinung, M., Stöver, T., Baumann, U., & Rader, T. (2015). Hearing preservation and improved speech perception with a flexible 28-mm electrode. Otol Neurotol. 2015 Jan;36(1):34-42.
- Müller, J., Brill, S., Hagen, R., Moeltner, A., Brockmeier, S.J., Stark, T., Helbig, S., Maurer, J., Zahnert, T., Zierhofer, C., Nopp, P., & Anderson, I. (2012). Clinical trial results with the MED-EL fine structure processing coding strategy in experienced cochlear implant users. ORL J Otorhinolaryngol Relat Spec., 74(4), 185–198.
- Roy, A.T., Carver, C., Jiradejvong, P., & Limb, C.J. (2015). Musical sound quality in cochlear implant users: A comparison in bass frequency perception between Fine Structure Processing and High-Definition Continuous Interleaved Sampling Strategies. Ear Hear., 36(5), 582–590.
- Roy, A.T., Penninger, R.T., Pearl, M.S., Wuerfel, W., Jiradejvong, P., Carver, C., Buechner, A., & Limb, C.J. (2016). Deeper cochlear implant electrode insertion angle improves detection of musical sound quality deterioration related to bass frequency removal. Otol Neurotol., 37(2), 146–151.
- Kleine Punte, A., De Bodt, M., & Van de Heyning, P. (2014). Long-term improvement of speech perception with the Fine Structure Processing coding strategy in cochlear implants. ORL, 76, 36–43.



CTA Form Success Message
Send us a message
Field is required
John Doe
Field is required
name@mail.com
Field is required
What do you think?
The content on this website is for general informational purposes only and should not be taken as medical advice. Please contact your doctor or hearing specialist to learn what type of hearing solution is suitable for your specific needs. Not all products, features, or indications shown are approved in all countries.